Hearing the words “You may need tests to rule out cancer” can be overwhelming. Patients often ask: Which tests will I need? Why are scans important? Is a biopsy always necessary? These are valid concerns.
Diagnosing head and neck cancers is not based on a single scan or symptom. It involves a careful process of clinical examination, imaging, tissue testing, and staging to understand the exact location, size, and spread of the disease. Accurate diagnosis is the foundation for choosing the right treatment and improving outcomes.
In this article, I explain how head and neck cancers are diagnosed, what different tests mean, and why each step matters.
What Are Head & Neck Cancers?
Head and neck cancers refer to cancers that develop in areas such as:
- Mouth (oral cavity)
- Tongue
- Throat (pharynx)
- Voice box (larynx)
- Nasal cavity and sinuses
- Salivary glands
- Thyroid gland
- Jaw or facial regions
- Neck lymph nodes
Early diagnosis significantly increases treatment success and may reduce the need for extensive surgery.
When Should You Seek Evaluation?
Certain symptoms should not be ignored, especially if they persist for more than 2–3 weeks:
- Non-healing mouth ulcers
- Persistent sore throat
- Difficulty swallowing
- Hoarseness or voice changes
- Lump in the neck
- Unexplained bleeding from mouth or nose
- Persistent ear pain
- White or red patches in the mouth
- Difficulty opening the mouth
- Weight loss without clear reason
Not all symptoms indicate cancer, but persistent signs require specialist evaluation.
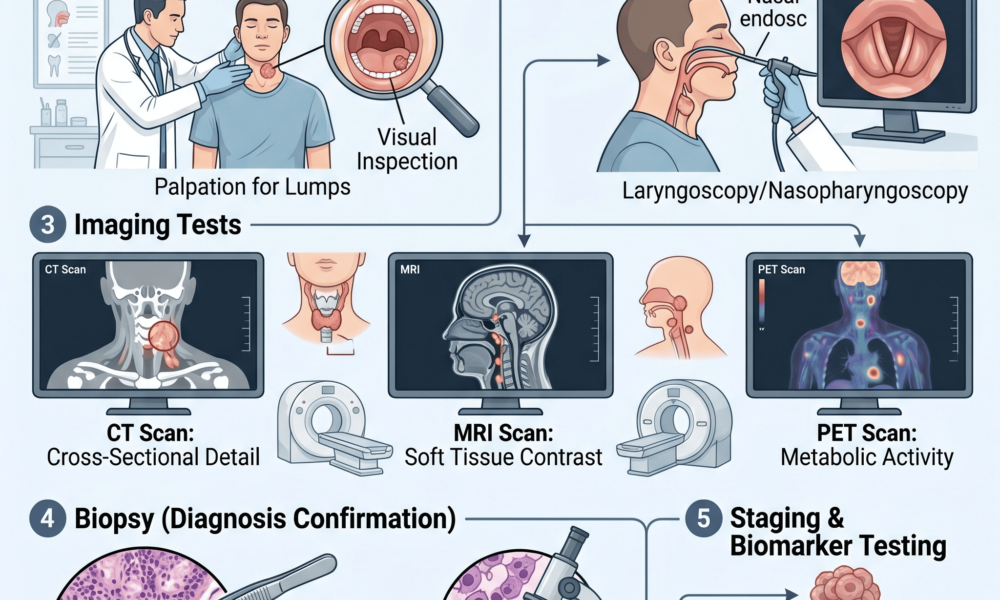
Step 1: Detailed Medical History & Clinical Examination
Diagnosis begins with understanding:
- Symptoms and duration
- Tobacco, alcohol, or supari use history
- Previous illnesses
- Family history
- Weight changes
- Swallowing or breathing issues
A thorough physical examination includes checking:
- Mouth and tongue
- Neck lymph nodes
- Throat
- Voice box
- Nasal passages
Many abnormalities can be identified during an experienced clinical examination.
Step 2: Endoscopy – Looking Inside Hidden Areas
Some tumors cannot be seen directly during routine examination. Endoscopy helps visualize deeper regions.
Types may include:
Flexible Nasoendoscopy
A thin camera passes through the nose to examine:
- Nose
- Throat
- Voice box
Laryngoscopy
Used for evaluating:
- Vocal cords
- Larynx
- Upper airway
Panendoscopy
Sometimes performed under anesthesia to inspect multiple regions comprehensively.
Patients often worry about discomfort; most office-based endoscopies are quick and well tolerated.
Step 3: Imaging Tests – Understanding the Extent of Disease
Scans help determine:
- Tumor size
- Exact location
- Involvement of surrounding structures
- Lymph node spread
- Distant metastasis
Different imaging techniques serve different purposes.
CT Scan (Computed Tomography)
A CT scan provides detailed cross-sectional images.
Useful for:
✓ Bone involvement
✓ Tumor size assessment
✓ Neck lymph node evaluation
✓ Surgical planning
CT scans are commonly recommended in oral cancers and advanced tumors.
MRI Scan (Magnetic Resonance Imaging)
MRI provides better soft tissue detail than CT in certain situations.
Helpful for:
- Tongue cancers
- Skull base tumors
- Soft tissue involvement
- Nerve-related spread
MRI can define boundaries that influence treatment planning.
PET-CT Scan
PET-CT combines metabolic imaging with anatomical imaging.
Often used for:
- Detecting hidden spread
- Advanced-stage cancers
- Assessing recurrence
- Treatment response evaluation
PET scans are not necessary for every patient.
Ultrasound
Neck ultrasound may help assess:
- Thyroid nodules
- Salivary gland lesions
- Neck lymph nodes
Ultrasound-guided procedures can also improve biopsy accuracy.
Step 4: Biopsy – The Most Important Diagnostic Test
A scan may suggest cancer, but biopsy confirms the diagnosis.
A biopsy involves removing a small tissue sample for microscopic examination.
This determines:
- Whether cancer is present
- Cancer type
- Tumor characteristics
- Grade of disease
Without tissue diagnosis, treatment decisions remain incomplete.
Types of Biopsy
Incisional Biopsy
Small tissue sample taken from suspicious lesions.
Common in:
- Mouth ulcers
- Tongue lesions
- Oral cancers
Fine Needle Aspiration Cytology (FNAC)
A thin needle extracts cells from:
- Neck lumps
- Lymph nodes
- Salivary gland masses
- Thyroid nodules
FNAC is minimally invasive.
Core Needle Biopsy
Obtains a larger tissue sample than FNAC.
Useful when additional tissue analysis is needed.
Excisional Biopsy
Entire suspicious lesion is removed for testing.
Step 5: Pathology Report – Understanding the Results
After biopsy, pathologists evaluate:
- Cancer type
- Tumor grade
- Aggressiveness
- Margins (if removed)
- Molecular features (in selected cases)
Common diagnoses include:
- Squamous cell carcinoma
- Thyroid cancers
- Salivary gland cancers
- Lymphomas
The pathology report strongly influences treatment recommendations.
Step 6: Cancer Staging
After diagnosis, staging determines how advanced the cancer is.
Staging considers:
T: Tumor size
N: Lymph node involvement
M: Spread to distant organs
This TNM system helps classify disease stages:
- Stage I
- Stage II
- Stage III
- Stage IV
Importantly, stage IV does not always mean untreatable. Many advanced cancers can still be managed effectively with surgery, radiation, targeted therapy, or multimodality treatment.
Why Accurate Diagnosis Matters Before Treatment
Starting treatment without complete evaluation may lead to:
- Incorrect treatment planning
- Incomplete surgery
- Missed spread
- Increased recurrence risk
Modern cancer care relies on precise diagnosis before deciding between:
- Surgery
- Radiation therapy
- Chemotherapy
- Immunotherapy
- Targeted therapy
- Combined treatment approaches
Common Questions Patients Ask
Is one scan enough to diagnose head & neck cancer?
No. Imaging suggests abnormalities, but biopsy confirms diagnosis.
Is biopsy dangerous?
Biopsy is generally safe and essential for treatment planning.
Are scans painful?
Most imaging tests are painless. Some require contrast injections.
Can cancer be diagnosed early?
Yes. Early evaluation of persistent symptoms increases chances of diagnosis at a treatable stage.
Final Thoughts
A diagnosis of head and neck cancer is rarely based on one test alone. It requires combining clinical examination, imaging, endoscopy, and tissue diagnosis to understand the disease fully.
Early detection often means simpler treatment, better outcomes, and improved quality of life. Persistent symptoms should never be ignored.
If you experience unexplained mouth ulcers, neck swelling, voice changes, or swallowing difficulties, seeking specialist evaluation early can make a significant difference.
About Oncologist
Dr. Dushyant Mandlik is an experienced Best Head & Neck Cancer Surgeon in ahmedabad specializing in diagnosis, surgical treatment, reconstruction, and comprehensive care for patients with oral cancer, thyroid cancer, salivary gland tumors, and other head & neck cancers. His focus is on evidence-based treatment, precision surgery, and patient-centered cancer care.